BACK · MAP · BYBERRY PICS · PATIENT HANDBOOK · MAIN MENU
A Brief History of Byberry
Introduction
The following is taken directly from a report filed approximately 1962 after the conduction of an anthropological study of the then new Rehabilitation Unit of the Eastern State Hospital (Byberry). The report is far from complete though we have managed to gather about one half of the full text, including the first two sections in their entirety. The report discusses the cultural conditions of the hospital administration more so than the patients' living conditions, but as such offers a glimpse into the nature of Byberry, how it functioned, and why it had the reputation it did almost since its inception. Below are the first two sections copied verbatim detailing, if somewhat briefly, the history of the hospital as of approximately 1960.
The Philadelphia Hospital for Mental Diseases officially began operations in 1912 as a place for those afflicted with diseases of the mind could live out a healthy, productive life. In keeping with psychiatric philosophy at the time the hospital quickly took on the roll of a custodial institution - an overcrowded warehouse for the incurable. At one point the report, written by an unknown anthropologist, estimates that as many as 86% of the hospital's admissions were patients that had been treated - some multiple times - at other hospitals and were being dispatched to Byberry as something of a 'last resort.' The report does not delineate whether these patients come to Byberry as a result of being branded incurable by other institutions, or if they their private funds ran out and were no longer welcome at the private institutions that previously housed them.
The report also discusses the nature of the employees of Byberry. For a long time - during the hospital's term under city control - interns were hired without any training or significant selection process. The hospital was desperate for workers willing to deal with the hospital's conditions for the meager pay that the city was willing to offer. Thus the staff was fraught with drunks, transients and otherwise unemployables. The treatment that these individuals gave the patients - in concert with the seemingly inhumane therapy methods of the time - created a popular conception about the facility that was, while based in reality, exaggerated.
Much of the public awareness about Byberry stemmed from a series of undercover investigations performed by the pro-labor J. David Stern owned newspaper The Philadelphia Record. Reporters like Mac Parker had an easy time getting hired by the hospital in order to get inside to document the living conditions. These were groundbreaking expos�s that piqued public interest in the institution throughout the 1930�s. Several Grand Jury investigations probed into the administration and conditions of the hospital, but impeded by political obstruction by the then dominant Republican party, little came of the juries� findings beyond minor patches and fixes by the W.P.A. (A depression era public works program). It was not until 1938, with mayor S. Davis Wilson distracted by growing union unrest within the city, his own bid for a US Senate seat, and his failing health, that control was wrenched away into the hands of The Commonwealth in an effort lead by PA Sen. Harry Shapiro and the long since defunct Philadelphia Record.

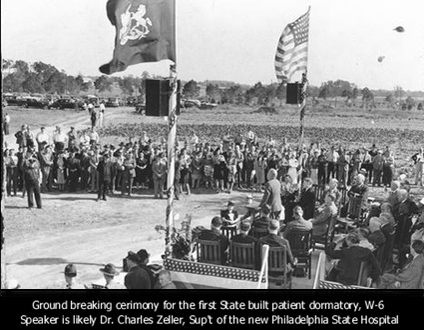
A new Superintendent, Dr Charles Zeller (formerly of Fairview State Hospital) was named, along with a new Board of Trustees (which included Sen. Shapiro). The transfer and subsequent rebirth of the hospital was overseen by the superintendents of several nearby psychiatric institutions including Dr. A Noyes of Norristown State Hospital, Dr. H Woolley of Pennhurst and Zeller himself. For many this seemed to signal the coming of a golden age for the Hospital, and psychiatric care in the City of Philadelphia.
Despite change in ownership from City to State in September of 1938, and the subsequent construction of several modern patient's wards, research and medical facilities, the hospital retained its reputation as a last resort asylum. Unfortunately, this was not without merit. This report discusses internal administrative strife, infighting between Physicians', Pshchologists' and Nurses' departments - each attempting to secure greater power and autonomy for itself within the hospital administration, shullfing patients back and forth in an effort to show significant progress on paper - in an effort to further their own agendas. It seems understandable then that the patients would turn up the worse for all this political struggle. Often times the people who were closest to the patients, the interns and orderlies had no input into the direction of an individual's care - and worse yet were subjected themselves to a system of 'multiple subordination' answerable to each of the competing departments. It follows easily that even the most dedicated and well meaning employees would soon fall under a cloud of malaise and entropy, while less than enthusiastic employees could fall into habits begetting patient neglect and abuse.
Byberry was, throughout its history, the subject of one investigation after another - almost continuously under the microscope by one of a host of governmental agencies or special interest groups. Public misunderstanding of psychiatric therapies, underfunding, misadministration and alleged staff abuses of patients kept Byberry in a negative light. Byberry was not alone in this, as the age of deinstitutionalism dawned in the 1950�s - coincident with the introduction of chlorpromazine (or Thorazine in the US) and related neuroleptics.
It is with little surprise that we see, beginning in the 1960's, the steady downsizing of The Hospital. In the 1970's the movement began to gain significant momentum in the United States away from Institutionalized care for non-chronic patients. Aided greatly by the introduction of a myriad of psychotropic medications, �Community Mental Health Centers� began to emerge as the preferred way of dealing with those with afflictions of the mind. Their lower cost approach to treatment and reimmersion of patients into the 'real world' appealed to budget concious legislators. Thus they also started consuming a greater and greater portion of the public mental health budget - leaving less for giant institutions like Byberry.
The Community Mental Health Centers, who initially dealt almost exclusively with acute curable patients, began to show encouraging success - while the institutions who were left with the long-term chronic and incurable patients were unable to show any levels of rehabilitation or returning their patients to society. This drove the last nail in the coffin for giant hospitals like Byberry. As the state continued to shift its spending from Hospitals to federally subsidized half-way houses, Byberry was forced to cede more and more patients either to other institutions or to the community centers. In this doomed state Byberry finally closed it's doors in 1990 shifting it's remaining patients either to Norristown State Hospital or to the very community centers who were stealing its funding.
An Anthropological Study of the Rehabilitation Unit of The Philadelphia State Hospital
Pt 1. A Bit of History
The Philadelphia State Hospital, a mental institution with approximately 6500 patients and 1300 staff members, is located on the northeast boundary of Philadelphia, Pennsylvania about 20 miles from the center of the city. A city run hospital for 32 years, the Commonwealth of Pennsylvania assumed control in 1938, and the institution has been state controlled and operated since. The patient buildings (numbering more than 30) and the various maintenance buildings (laundries, laboratory, power plants, etc.) are situated on 1,000 in an area called Byberry, with an additional 500 acres maintained for farm purposes across the county line in Bensalem Township.
This is a far cry from the humble beginning of what is now The Philadelphia State Hospital. An 1883 report of the Board of Public Charities noted that "...a very large proportion of the class that has been styled the criminal (sic) insane are confined either in jails, prisons or almshouses, none of which are provided with the means for proper care and treatment for this afflicted portion of our people." In 1885, when fire destroyed the Insane Department of the Blockley Almshouse, a forerunner of the present Philadelphia General Hospital, the committee on Lunacy campaigned for a mental institution separate in administration and location from the almshouse, with adequate facilities for the mentally ill.
Thoughts turned to Byberry, in the far northeast corner of the city, and finally in 1906, a physician from the insane department from the Philadelphia General Hospital arrived with six male patients in the heart of what was then farm country. Several farms had been purchased for this purpose by the City of Philadelphia. The six patients worked under the guidance of a farmer and several attendants from the hospital. More patients were transferred there, and this was the beginning of 'Byberry,' the name of the locality having been unofficially applied to the hospital from the offset. "It's a farm colony, the medical care of which was under the care of Dr. H--- (sic) who visited the patients at least once a week. Later a Dr. B--- (sic) was placed in charge of the patients at Byberry." (quoted from a letter from Dr. W G Bowers - who attended the first six patients - to the then superintendent of Byberry c.1946) When sufficient buildings had been provided 2,000 patients from the Insane Department were transferred to Byberry. Only acute cases were detained at Philadelphia General Hospital, "... and if their stay was more than two or three weeks they were committed to Byberry..." (ibid) The Philadelphia Hospital for Mental Diseases (Byberry's official name from 1906 to 1938, while operated by the City of Philadelphia) had taken a great step towards being the very large institution The Philadelphia State Hospital is today.
Relatively little is known about the Hospital during the years of city control. There are reports of meager medical and psychiatric attention and maltreatment of patients, generally deplorable conditions, but it is not until the post 1938 period of state control that we have documented, reliable information about the social structure and culture of the Institution. The Philadelphia State Hospital, called by its popular and derogatory name, Byberry, was, and often still is, considered a Bedlam, a mad house where unspeakable behavior took place, on the part of the patients and the personnel. Once under state control, many of the rumored conditions were found to prevail, others were gross exaggerations. The characterization remains, however, of Byberry as a "dumping ground," where mentally deranged persons are sent, supposedly to safeguard the community. There is also the feeling, most often not verbalized, that such incarceration relieves relatives, friends, and the community from further consideration, from further involvement, from caring. "You mean to tell me people actually get out of there?" people will ask incredulously. "Aren't you afraid to work in such a place?" others ask. Although modern efforts at mental health education have made great strides the myth still generally prevails about Byberry as "that insane asylum where dangerous people are kept and from which no one is released."
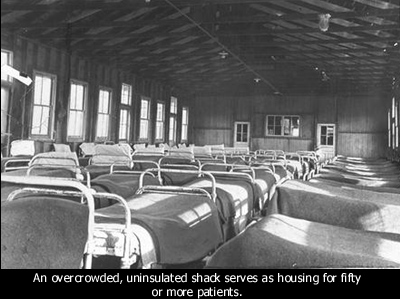
Conditions in the early years of state control were far from desirable. For example, one of the buildings was appropriately but indelicately called the "Rose Garden," a sarcastic reference to the stench about the place. Attendants, the employees who have the greatest involvement with patients, were frequently hired off the street. As one informant reported "We got drunks and everything else. We even had a sign on the Boulevard advertising for attendants and you can imagine what we got from that transient bunch. If they wanted the job, they got it. There was a big turn-over. Many attendants in those days were discharged for being drunk on duty."
Those were the days of restraints. Each building had sheet and pack restraints and the still persistent seclusion rooms. Patients were strapped to chairs by arms and feet. The great destruction of clothing and its consequent nakedness made such restraints necessary. Destroyed clothing simply could not be replaced, nor were there sufficient employees to perform this constant chore. Hundreds of patients were bare foot. This kind of situation, continuing to rather recent times, which prompted a 1945 Life Magazine pictorial expose, in which conditions at The Philadelphia State Hospital and other institutions were extensively noted and displayed.
The ugly past is not some odious relic which is forgotten or denied by the administration and personnel of the Hospital. The Superintendent retains copies of the Life article for his files and readily made them available - along with numerous other reports and records - to this investigator. They are kept as reminders of a past to be remembered, but never duplicated. They are discussed and displayed in the admitted hope that the public, on which the institution depends for its existence, will show enough interest to provide the staff, facilities, and materials essential to the proper functioning of the Hospital.
While there are institutional failings and inadequacies prevalent at the time of this writing - to be noted subsequently - the improvement in the conditions briefly described above has been quite remarkable. The following quotation, from the January 1950 issue of a now defunct hospital publication, The By-Line, presents an accurate account of the progress made in the first decade of state operation, with particular reference to new and improved buildings and plant: "More than eleven years have elapsed since the Commonwealth of Pennsylvania took over the administration of the Philadelphia State Hospital. During this period many changes have taken place; changes which have aided in eliminating the deplorable conditions then existing...
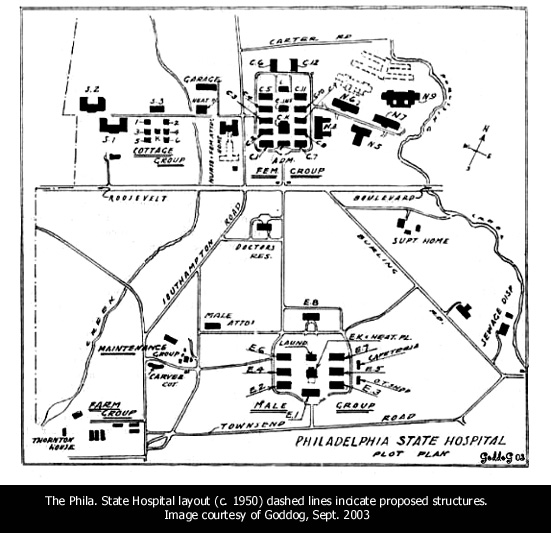
- "Where patients were formerly housed in dilapidated buildings, we now have such modern buildings as S-1, S-2, N-6 and N-7...
- "The dietary Dept. has vastly improved facilities with the addition of the N-5 kitchen, the Female Kitchen, and Central Dining Room. Two new buildings are in the process of being constructed. Plans for new Tuberculosis, Administration, Female Maximum Security and medical-Surgical Buildings are under way.
- "The additional 505 acres of farm which have been acquired in Bucks County, should greatly increase our 'home grown' food supply."
- "other notable changes have been: modern automotive equipment and garage, good surfaced roads, remodeled sewage disposal plant... Since 1939, the working conditions of our employees have been made more attractive by shorter working hours, increased pay, and more holidays. Improved training of our personnel is showing gratifying results..."